
Best Vitamin B12 for Nerve Damage: Methylcobalamin vs Cyanocobalamin
My neurologist checked my B12 during a routine panel two years into my neuropathy diagnosis. It came back “within normal range.” She moved on. I didn’t.

What I found when I started digging: “normal range” for B12 is notoriously wide, and the form of B12 your body actually uses for nerve repair is not what most supplements contain. The difference matters more than most people realize.
Key Takeaways
- 64% of diabetic peripheral neuropathy patients show altered B12 levels compared to only 17% without neuropathy (PubMed, 2025).
- Methylcobalamin is the active form that crosses into the nervous system and is directly usable by nerve cells.
- Methylcobalamin accounts for 90% of cobalamin found in cerebrospinal fluid (PMC, 2024).
- 1,000 mcg/day of methylcobalamin for 12 months improved neurophysiological parameters in diabetic neuropathy patients in a controlled trial.
Why Does Vitamin B12 Matter for Nerve Damage?
Nearly 80% of patients with neurologic B12 deficiency show evidence of peripheral neuropathy (Medscape, 2024). B12 is not optional for your nervous system. It’s foundational.
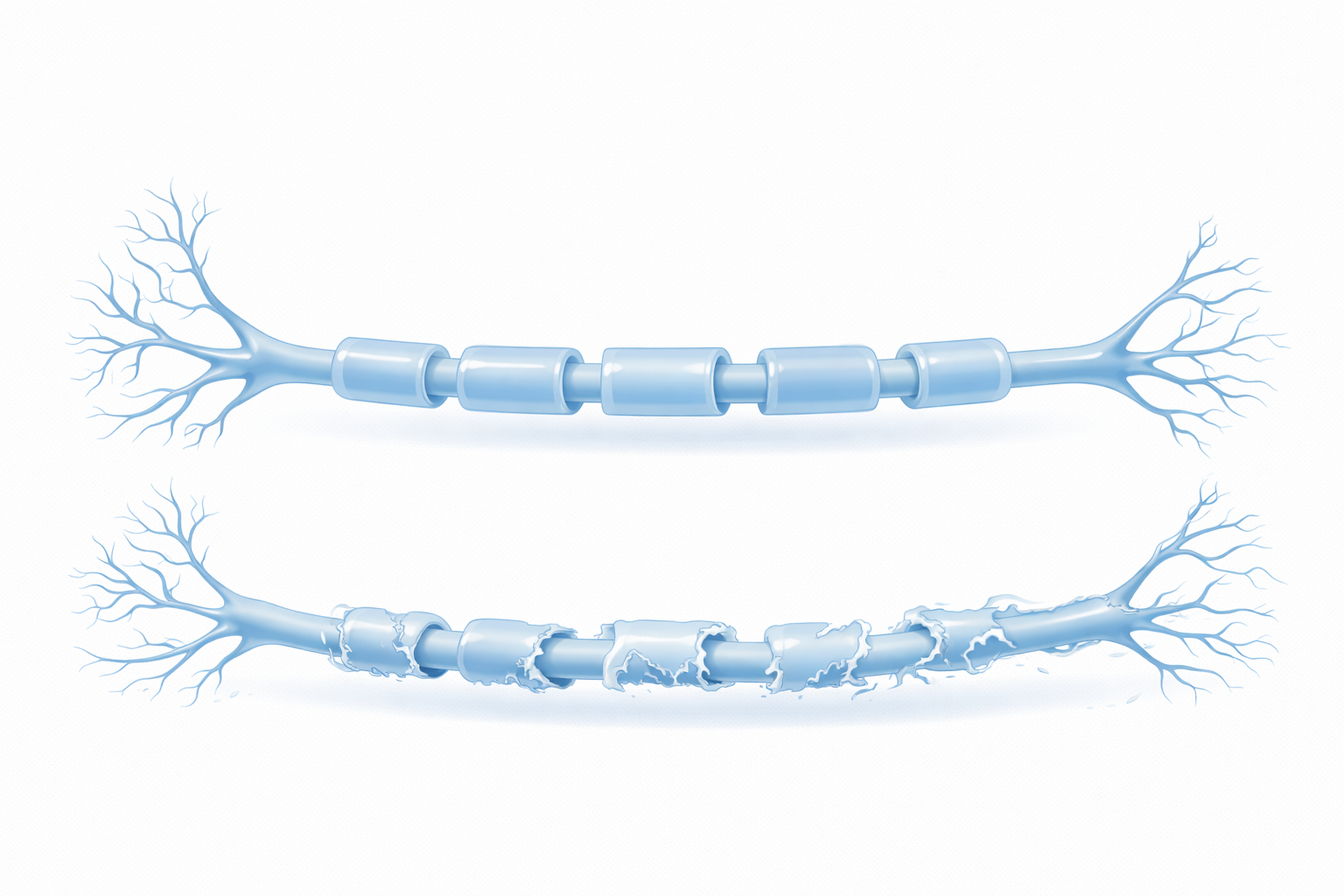
Your nerve fibers are wrapped in a protective sheath called myelin. B12 is required for myelin synthesis. Without adequate B12, that sheath degrades. Signals slow down or misfire. You get the burning, tingling, and numbness that anyone with peripheral neuropathy knows too well.
B12 also participates in the production of S-adenosylmethionine (SAM-e), which your body uses to repair DNA and support the methylation cycle. When methylation is impaired, nerve cell regeneration slows.
The problem isn’t just outright deficiency. Studies consistently show that even low-normal B12 levels, values your doctor might not flag, are associated with worse neuropathy outcomes. And 15 to 40% of older adults have low serum B12, with 5 to 20% meeting full deficiency criteria.
My levels read 287 pg/mL. My doctor called it fine. The research I found suggested that neurological symptoms can appear with levels below 400 pg/mL. I started supplementing. Three months later, I retested at 612 pg/mL. My morning burning was not gone, but it was meaningfully less.
Methylcobalamin vs Cyanocobalamin: What’s the Real Difference?
Methylcobalamin is the biologically active form of B12. Cyanocobalamin is synthetic. Your body must convert cyanocobalamin before it can use it, and that conversion requires several enzymatic steps that become less efficient with age, gut issues, or genetic variants like MTHFR.
Methylcobalamin accounts for 90% of the cobalamin found in human cerebrospinal fluid (PMC, 2024). That single statistic tells you which form the nervous system prefers.
Why Cyanocobalamin Falls Short for Nerve Repair
Cyanocobalamin is cheaper to manufacture, more stable on a shelf, and is the form used in most mass-market B12 supplements and fortified foods. It works adequately for people who just need to prevent basic deficiency. For nerve repair, it has two problems.
Conversion dependency. People with MTHFR mutations, estimated at 10 to 15% of the population, convert cyanocobalamin to usable B12 inefficiently. They may show normal serum B12 while remaining functionally deficient at the cellular level.
The cyanide molecule. Cyanocobalamin contains a small cyanide group that your body must remove before using the B12. The amount is not dangerous for most people, but it adds a metabolic step and makes cyanocobalamin unsuitable for anyone with kidney disease or impaired detoxification.
Why Methylcobalamin Is the Better Choice for Neuropathy
Methylcobalamin is already in the form your nerves can use. It crosses the blood-brain barrier more readily than cyanocobalamin. It’s retained in tissues at higher concentrations. And it’s the form used in most of the clinical research showing neurological benefit.
One detail rarely mentioned: methylcobalamin also provides methyl groups your body uses for neurotransmitter synthesis. This means it may support mood and cognitive function alongside nerve repair, a meaningful benefit for anyone dealing with the depression and brain fog that often accompany chronic pain.
What Does the Research Show About B12 and Nerve Repair?
A 2024 meta-analysis published in PMC found that methylcobalamin monotherapy and combination therapy were both more effective than control groups, with zero serious adverse events reported (PMC, 2024). The effect sizes were consistent across diabetic neuropathy, chemotherapy-induced neuropathy, and idiopathic peripheral neuropathy.
A 12-month controlled trial using 1,000 mcg/day of oral methylcobalamin in diabetic neuropathy patients showed significant improvements in nerve conduction velocity, vibration perception threshold, and quality of life scores (PubMed, 2021). Nerve conduction velocity is measured objectively, the nerves were functioning better.
A 2025 study found that combining B1 (thiamine), B6 (pyridoxine), and B12 (methylcobalamin) produced superior neural cell maturation and connectivity compared to individual vitamins alone (PubMed, 2025). The combination approach amplifies what each B vitamin does independently.
For severe cases, high-dose IV methylcobalamin, 25 mg/day for 10 days followed by monthly maintenance doses, has been shown safe and effective for chronic axonal degeneration (PubMed, 2014). This is well above oral supplementation levels and requires medical supervision.
What’s the Right Dose of Methylcobalamin for Neuropathy?
The research does not support a single universal dose, but here’s what the clinical literature shows.
For maintenance and deficiency prevention: 500 to 1,000 mcg/day oral methylcobalamin is what most studies use as a baseline and what’s typically recommended for neurological support.
For active nerve repair: Several trials use 1,500 to 3,000 mcg/day. Higher doses are especially relevant when gut absorption is compromised, which is frequent in diabetics and older adults due to reduced intrinsic factor production.
Sublingual vs oral: Sublingual methylcobalamin dissolves under the tongue and reaches the bloodstream directly, bypassing the gut entirely. For anyone with digestive issues, low stomach acid, or a history of gastric surgery, sublingual is significantly more reliable than swallowing a tablet.
I take 1,500 mcg sublingual methylcobalamin each morning, before food. My current B12 level is 712 pg/mL. My neurologist, who previously didn’t mention B12 at all, now asks what I’m taking.
Should You Combine B12 With Other Supplements for Neuropathy?
Yes, with caveats. B12 works better in context. The 2025 combination study found that B1+B6+B12 outperformed any single B vitamin (PubMed, 2025). If you’re only taking B12, you may be leaving results on the table.
Folate, specifically methylfolate, not folic acid, is also relevant. B12 and folate work together in the methylation cycle. Taking high-dose B12 without adequate folate can mask a folate deficiency in blood tests while the deficiency continues causing harm.
Alpha lipoic acid has solid clinical evidence for neuropathy relief and pairs well with B12. It reduces oxidative stress in nerve cells through a different mechanism, making the combination additive rather than redundant.
For a comprehensive supplement strategy that goes beyond individual vitamins, Arialief combines multiple neuropathy-targeted compounds in research-supported doses. I reviewed it in detail on this site, it includes B12 alongside other actives that address the oxidative and inflammatory components of nerve damage simultaneously. See my full Arialief review for the breakdown.
Affiliate disclosure: I receive a commission if you purchase through my Arialief link. This does not affect my assessment.
Frequently Asked Questions
Is methylcobalamin better than cyanocobalamin for neuropathy?
For nerve damage specifically, yes. Methylcobalamin accounts for 90% of the cobalamin in cerebrospinal fluid and is used directly by nerve cells without conversion. Cyanocobalamin requires enzymatic processing that becomes less efficient with age and is impaired in people with MTHFR mutations.
How long does it take for B12 to help neuropathy?
Clinical trials showing significant neurophysiological improvement used 12-month protocols (PubMed, 2021). Symptom improvements can appear earlier, sometimes within 8 to 12 weeks, but measurable nerve function changes take longer. Expect months, not days.
Can you take too much B12?
B12 is water-soluble and excess is excreted in urine. Toxicity at supplemental doses is not documented in the literature. Very high serum B12 without supplementation can indicate an underlying condition worth investigating, but the supplement itself is not dangerous at typical doses.
What’s the difference between sublingual and oral B12?
Sublingual B12 dissolves under the tongue and absorbs through mucous membranes, bypassing the digestive system. Oral tablets depend on intrinsic factor in the stomach, which declines significantly with age and is often impaired in diabetics. Sublingual is more reliable for anyone over 50 or with digestive issues.
Does B12 alone reverse neuropathy?
No. Neuropathy has multiple drivers, oxidative stress, poor circulation, glycemic damage, inflammation, and no single supplement addresses all of them. B12 specifically supports myelin repair and nerve cell regeneration. It works best as part of a broader approach. See my guide on natural ways to relieve neuropathy pain for the full picture.
Conclusion
The short answer: choose methylcobalamin over cyanocobalamin if nerve repair is your goal. The form matters. The dose matters. The delivery method matters, especially if you’re over 50 or have any digestive compromise.
B12 won’t fix neuropathy on its own. But if you’re deficient, even borderline deficient, it’s likely holding your recovery back. Get your levels tested. Aim for a serum B12 above 500 pg/mL. Start with 1,000 to 1,500 mcg/day sublingual methylcobalamin and retest in 90 days.
For a broader supplement approach that combines B12 with other evidence-backed compounds, my Arialief review covers what’s in it and how it compares. And for the full guide to supplements for peripheral neuropathy, I’ve ranked the options by evidence strength.
Medical Disclaimer: The information in this article is for educational purposes only and does not constitute medical advice. Mark Whitfield is not a medical professional. Always consult your physician before starting any supplement regimen, especially if you take medications or have a chronic health condition.





